

Med info
Congenital cataracts in children: early diagnosis and modern treatment options

What Is Congenital Cataract in Children?

Congenital cataract in children is a clouding or opacity of the eye’s natural lens that is present at birth or develops within the first months of life. This cloudiness leads to blurred or reduced vision and may cause amblyopia (lazy eye) or even permanent vision loss if not treated early.
It is considered one of the major causes of visual impairment in children. Congenital cataracts can result from genetic disorders, abnormal eye development in the womb, maternal viral infections during pregnancy such as rubella (German measles), or various congenital metabolic and systemic diseases.
The condition may affect one eye (unilateral) or both eyes (bilateral), and its severity can range from a mild opacity that has little effect on vision to a dense cataract that blocks light from reaching the retina altogether.
Parents may notice a white or grayish reflex in the pupil, eye misalignment (strabismus), or that the child does not visually track objects or respond to light in a way that would be expected for their age.
Early detection of congenital cataract and prompt assessment by a pediatric ophthalmologist are crucial to protect the child’s vision and maximize their chances of developing the best possible visual function.
The Difference Between Congenital and Acquired Cataracts
Understanding the difference between congenital and acquired cataracts in children is crucial for early detection and timely treatment.
Congenital cataract refers to lens opacity that is present at birth or appears within the first few months of life. It is often associated with genetic factors, maternal viral infections during pregnancy, or metabolic disorders. It may affect one eye or both and can lead to severe visual impairment if not treated promptly.
Acquired cataract, on the other hand, develops after birth, usually at a later age. It can result from eye injuries, the use of certain medications such as corticosteroids, or systemic diseases like diabetes. It typically develops gradually and presents with symptoms such as blurred vision or increased sensitivity to light.
Congenital cataracts are particularly critical in terms of visual development because they interfere with the formation of visual pathways in the brain during the early, sensitive years of childhood. For this reason, they require early diagnosis and rapid surgical intervention, in contrast to acquired cataracts, which usually progress more slowly and can often be managed with more stepwise treatment plans.
Recognizing this distinction helps parents understand the importance of newborn eye examinations and the need to monitor any abnormal signs in vision or eye movements, so that congenital cataracts can be detected before they lead to permanent amblyopia (lazy eye).
Who Is at Higher Risk?

Family History of the Disease
Children with a family history of congenital cataracts or early-onset cataracts fall into a higher-risk group for developing this condition.
When a parent or sibling has congenital cataracts, the likelihood of passing on a genetic predisposition to the child increases, even if the disease does not present with the same severity.
For this reason, a family history of congenital cataracts is considered an important warning sign that prompts the ophthalmologist to monitor the child closely from the first days or months of life, and to perform regular eye examinations to detect any lens opacity early, before it interferes with visual development.
Premature Birth
Preterm infants (born before 37 weeks of gestation) are at higher risk of developing congenital cataracts and other eye problems in general.
This is because the eye and the crystalline lens may not be fully developed at the time of premature birth. In addition, certain medical conditions or treatments in the neonatal intensive care unit (such as oxygen deficiency or specific medications) can further increase the risk of lens opacification.
Therefore, premature babies require early and regular ophthalmic examinations, as early detection of congenital cataracts is crucial to preserving visual function and minimizing the risk of permanent visual impairment.
Maternal Infection During Pregnancy
When the mother contracts certain viral or bacterial infections during pregnancy, the fetus becomes more prone to developing congenital cataracts.
Key examples include rubella, herpes, varicella (chickenpox), toxoplasmosis, and cytomegalovirus (CMV). These pathogens can disrupt normal lens development in utero and lead to congenital lens opacities.
For this reason, pregnant women are advised to adhere to recommended vaccination schedules, maintain regular antenatal follow-up with their obstetrician, and promptly treat any infections, in order to reduce the risk of congenital cataracts and other ocular disorders in the fetus.
Genetic Disorders and Congenital Syndromes
Infants with certain inherited diseases or congenital syndromes are at significantly increased risk of congenital cataracts.
These include, for example, Down syndrome, some inborn errors of metabolism such as galactosemia, as well as chromosomal and endocrine disorders.
In such conditions, cataracts often represent one component of a broader clinical picture. Consequently, physicians routinely examine the eyes of any child known to have a syndrome or genetic disorder associated with lens opacities.
Early and ongoing follow-up allows timely management of congenital cataracts and improves the child’s chances of developing the best possible visual function.
Symptoms of Congenital Cataracts in Children
Congenital cataracts usually become evident within the first days or months of life, and may affect one eye or both.
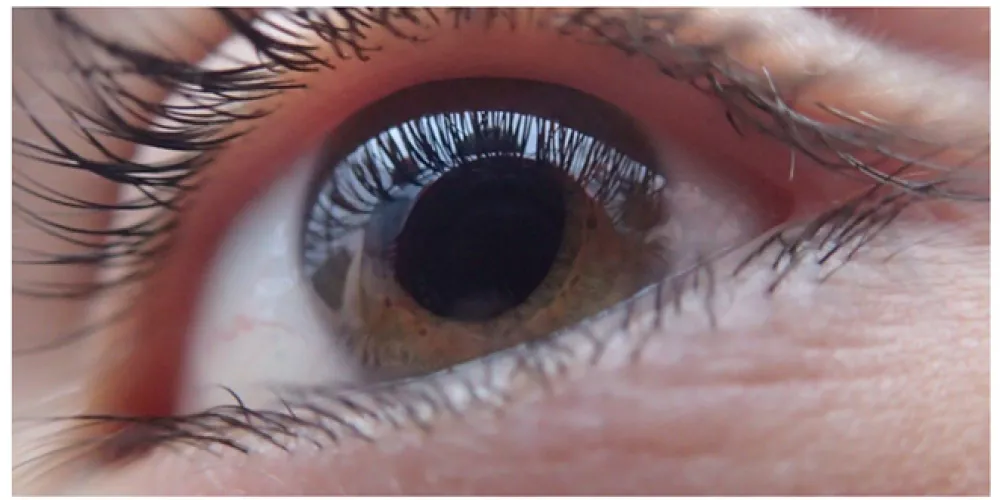
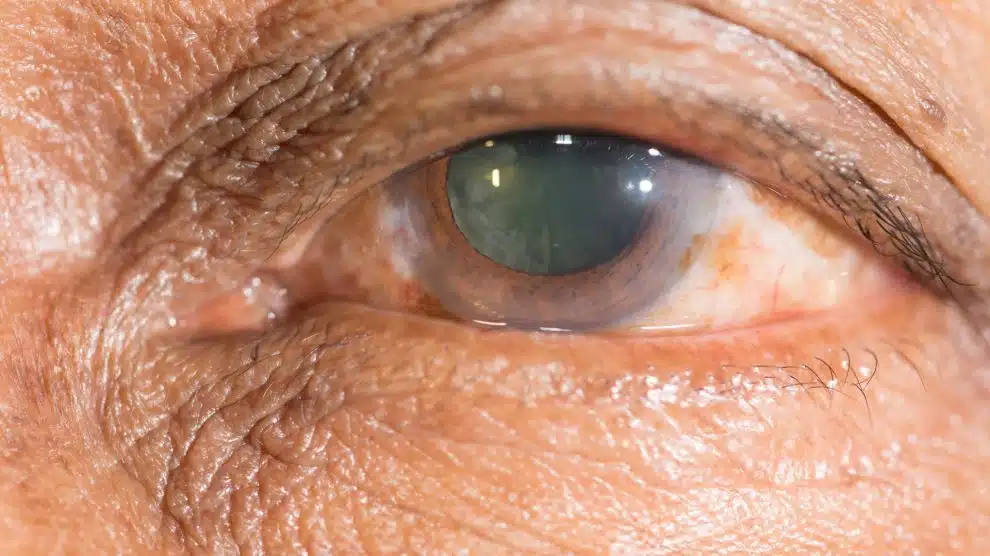
The main sign parents tend to notice is a white or cloudy appearance in the pupil instead of its normal black color, or a white reflex in photographs instead of the usual red reflex.
Parents may also observe that the baby does not make eye contact, doesn’t fixate on faces or colorful toys, and doesn’t follow moving objects with their eyes like other babies of the same age, which can indicate poor vision.
Other signs of congenital cataracts include eye misalignment (strabismus, where one or both eyes turn inward or outward), frequent blinking, marked sensitivity to bright light, and sometimes involuntary, repetitive eye movements (nystagmus).
The child may also be unusually irritable and cry often due to difficulty seeing, or show delayed visual and motor development, such as trouble reaching for or grasping small toys.
Noticing any of these symptoms warrants an urgent evaluation by a pediatric ophthalmologist, as early diagnosis and treatment of congenital cataracts are crucial to prevent permanent visual impairment and amblyopia (lazy eye).
How Is Congenital Cataract Diagnosed?
Red Reflex Examination
The red reflex test is one of the earliest and most important steps in diagnosing congenital cataracts in children. It is usually performed shortly after birth using a simple device similar to a small torch (ophthalmoscope).
The ophthalmologist or pediatrician shines a light into the baby’s eyes and observes the color reflected from the back of the eye. Under normal conditions, a uniform, bright red reflex is seen. When there is lens opacity, such as a congenital cataract, the reflex appears diminished, whitish, or irregular.
This quick, painless test enables early detection of lens opacity, which facilitates the diagnosis of congenital cataracts in children and allows timely planning of follow‑up or treatment.
Fundus Examination (Ophthalmoscopy)
Fundus examination is a key step in evaluating a child suspected of having a congenital cataract, as it allows the physician to visualize the retina, optic nerve, and intraocular blood vessels.
The pupil is first dilated using special eye drops, then the ophthalmologist uses lenses and magnifying instruments to carefully assess the internal ocular structures.
This examination helps distinguish congenital cataracts from other causes of opacity or reduced vision in children, and can reveal associated congenital anomalies or retinal diseases that may affect visual acuity and the overall management plan for congenital cataracts.
Ocular Ultrasound
Ocular ultrasound (B‑scan ultrasonography) is used when lens opacity prevents a clear view of the fundus, as in dense congenital cataracts.
The doctor gently moves a small probe over the eyelid or directly on the cornea after applying a special gel. The ultrasound waves generate detailed images of internal structures such as the lens, vitreous body, and retina.
This test helps assess retinal integrity and detect any internal abnormalities or retinal detachments, thereby improving the accuracy of diagnosing congenital cataracts in children and assisting in surgical planning when needed.
Examinations Under Anesthesia When Needed
In some cases—particularly in infants or non‑cooperative children—the ophthalmologist may opt to perform comprehensive examinations under light general anesthesia to ensure an accurate diagnosis of congenital cataracts.
Anesthesia allows the physician to measure intraocular pressure and examine the cornea, lens, and fundus calmly and precisely without eye movement, in addition to performing crucial measurements such as axial length and the intraocular lens power required before surgery.
These examinations under anesthesia are considered safe when carried out in specialized centers, and they play a major role in developing an integrated treatment plan for congenital cataracts and achieving the best possible visual outcomes for the child.
Genetic Testing in Selected Cases
In certain cases of congenital cataracts—especially when there is a positive family history, involvement of both eyes, or associated congenital anomalies—the physician may recommend genetic testing.
These tests aim to identify mutations or hereditary disorders linked to congenital cataracts, helping to clarify the underlying cause, anticipate disease course, and provide genetic counseling for the family.
Genetic testing is a complementary component in the work‑up of complex cases of congenital cataracts in children and contributes to planning long‑term follow‑up for siblings and relatives who may be at increased risk.
When Is Intervention Needed, and Why Is Early Treatment So Critical?
Early intervention in cases of congenital cataract in children is crucial, because delaying treatment can lead to permanent visual impairment known as amblyopia or “lazy eye.” This type of damage cannot be reversed later, even if the cloudy lens is removed.
Evaluation and management are generally recommended as soon as any abnormal signs are noticed in the child’s eyes, such as a white pupil (leukocoria), involuntary eye movements (nystagmus), eye misalignment (strabismus), or poor response to light and surrounding objects.
Pediatric ophthalmologists usually advise prompt surgical intervention in dense congenital cataracts within the first weeks or months of life, because during this period the child’s brain is actively “learning to see.” Any obstruction to clear light entering the eye in this critical window can interfere with normal development of the visual pathways.
Early treatment of congenital cataract significantly improves the chances of achieving good vision and reduces the risk of complications such as strabismus, learning difficulties, and poor concentration at school.
Therefore, early detection and regular follow‑up with a pediatric ophthalmology specialist are the most effective ways to protect a child’s eyesight and support the healthiest possible visual development.
Treatment Options for Congenital Cataracts in Children
Lens Surgery (Lensectomy)
Surgical removal of the opacified lens is the cornerstone of managing congenital cataract in children, especially when the opacity involves the visual axis and threatens to cause amblyopia.
During this procedure, the ophthalmic surgeon removes the cataractous lens using fine microsurgical techniques tailored to the small size of the pediatric eye, while carefully minimizing complications and preserving the surrounding ocular structures.
The timing of lens removal is critical; delaying treatment of congenital cataract can result in permanent visual impairment, even after surgery.
Surgery is typically recommended when the congenital cataract is dense or involves the central visual axis, whereas mild, non‑central opacities may be managed with observation and/or spectacles.
Providing parents with a clear explanation of the risks and benefits is an essential part of the treatment plan for congenital cataract, to support an informed decision about proceeding with lens extraction.
Intraocular Lens (IOL) Implantation
Following removal of the opacified lens in congenital cataract, the ophthalmologist considers options to replace the eye’s refractive power, one of the key options being implantation of an intraocular lens (IOL) specifically designed for children.
Implanting an intraocular lens helps focus images accurately on the retina, thereby promoting better visual development and reducing the risk of amblyopia.
In very young children, an artificial lens is sometimes not implanted during the initial surgery; instead, contact lenses or glasses are used, with secondary IOL implantation considered at an older age, depending on ocular status and the child’s growth.
Selection of the IOL type and power is based on precise biometric measurements of the child’s eye and on a long‑term management strategy for congenital cataract, including anticipated need for spectacles and future vision therapy.
While IOL implantation can reduce dependence on thick spectacles, it requires regular follow‑up to detect potential complications such as elevated intraocular pressure or posterior capsular opacification.
General Anesthesia
Congenital cataract surgery in children is most often performed under general anesthesia to ensure the child remains completely still, providing optimal operative conditions for accurate lens removal and/or IOL implantation.
General anesthesia allows the procedure to be carried out safely without the child experiencing pain or fear, which can shorten operating time and improve surgical outcomes.
Before anesthesia, the child undergoes a thorough medical assessment to rule out conditions that might increase anesthetic risk, and all relevant details are discussed with the parents.
The anesthesia team works closely with the ophthalmic surgeon to continuously monitor the child’s vital signs during and after surgery, ensuring safe emergence from anesthesia and adequate postoperative pain control.
General anesthesia is a key component of the treatment strategy for congenital cataract in children, as it provides the ideal setting to perform highly delicate surgery on a small, sensitive eye.
Best Pediatric Congenital Cataract Specialist – Search-Optimized Medical Translation
Dr. Mohamed Jayed – One of the Leading Pediatric Congenital Cataract Specialists in Jeddah
Dr. Mohamed Jayed is widely regarded as one of the foremost ophthalmologists specializing in congenital cataract management in children in Jeddah. He combines extensive expertise in pediatric eye surgery with meticulous care for complex cataract cases.
He has broad clinical experience in the early diagnosis of congenital cataracts and in tailoring an individualized treatment plan for each child, taking into account age, cataract density, and its impact on vision.
Choosing a top specialist in congenital cataract in children, such as Dr. Mohamed Jayed, significantly improves the chances of preserving the child’s eyesight, minimizing complications, and achieving the best possible long‑term visual outcomes.
In his specialized clinic in Jeddah, Dr. Jayed relies on advanced diagnostic tools such as ultrasound B‑scan of the posterior segment and detailed lens assessment, helping determine the optimal timing for surgery as well as the most appropriate intraocular lens options for each case.
For parents seeking the best doctor to treat congenital cataracts in children in Jeddah, Dr. Mohamed Jayed is a highly trusted choice, known for his strong medical reputation and his commitment to close postoperative follow‑up to ensure the child’s visual development progresses appropriately.
What happens if congenital cataracts are not treated?
Leaving congenital cataracts untreated in children can lead to serious, permanent damage to their vision. When the lens remains cloudy and clear images cannot reach the retina, the child may develop amblyopia, commonly known as “lazy eye,” in which the brain gradually stops using the affected eye.
Over time, this visual impairment may become irreversible, even if the cataract is later removed, because the visual pathways in the brain do not develop normally during the critical early years of life.
In bilateral cases (when both eyes are affected), the child may experience severe visual impairment that negatively impacts motor and cognitive development, causes learning difficulties, and delays the acquisition of visual skills such as shape and color discrimination.
Untreated congenital cataracts can also increase the risk of strabismus (ocular misalignment), impaired depth perception, and loss of stereoscopic (3D) vision, all of which adversely affect the child’s quality of life and academic and social development.
Early diagnosis and prompt treatment are therefore essential to prevent functional blindness and to support normal visual development in the child.
Why Choose Batal Specialized Eye Center for Treating Congenital Cataracts in Children?
Batal Specialized Eye Center is considered one of the leading centers for managing congenital cataracts in children, thanks to its team of consultant pediatric ophthalmologists who are highly experienced in delicate cataract surgery performed under the highest safety standards.
The center relies on state-of-the-art diagnostic equipment to assess lens opacity, as well as retinal and optic nerve function in infants and children, enabling the development of a tailored treatment plan for each child.
Congenital cataract extraction and intraocular lens implantation are performed using advanced microsurgical techniques that shorten surgery time, promote faster recovery, and improve visual acuity in the long term.
The medical team prioritizes early intervention to prevent amblyopia and other complications related to poor vision, with meticulous follow‑up to monitor visual development and prescribe glasses or patching therapy when indicated.
Batal Specialized Eye Center also places great emphasis on educating parents about the signs of congenital cataracts, available treatment options, and follow‑up requirements, while providing a child‑friendly and safe environment that reduces anxiety and supports the treatment journey from diagnosis through to visual stabilization.





